

Running News Daily
Running News Daily is edited by Bob Anderson and team. Send your news items to bob@mybestruns.com Advertising opportunities available.
Index to Daily Posts · Sign Up For Updates · Run The World Feed



Is Reducing Inflammation Really the Best Way to Treat Running Injuries?

What is the role of inflammation in running injuries?
For a long time, inflammation has been identified as the main culprit for pain resulting from running injuries.
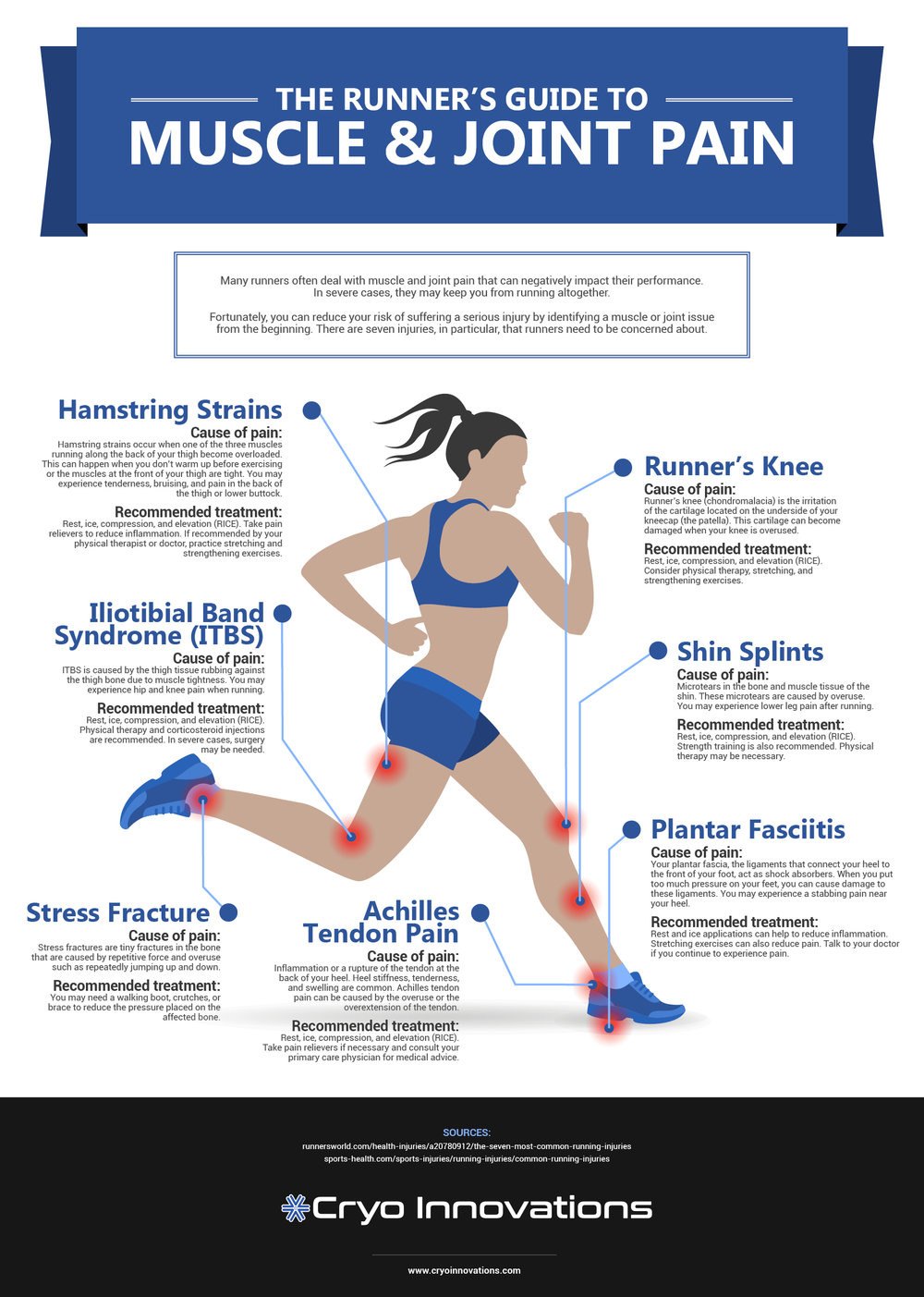
The inflammatory theory of running injuries asserts that, following minor damage from overuse to a muscle, tendon, or connective tissue, the body attacks the injured area with a rush of inflammatory cells which results in the pain, stiffness, and soreness at the injured site.
This inflammation has a detrimental effect on healing because the swelling and inflammation can cause secondary damage to the already-injured area.

To combat this, many treatments that have become mainstays of physical therapy offices and athletic training rooms are designed around reducing inflammation. This includes ice, anti-inflammatory drugs like ibuprofen, and compressive wraps.
But is this inflammatory model valid?
By definition, inflammation has features that are observable both on the macroscopic level of sensations in your body (like pain, redness, swelling—things a doctor would call “clinical features”), and on the microscopic level of the inner workings of your cells—this consists mainly of special inflammatory cells which flood an inflamed area and mediate your body’s response to the injury.
If the cause of the pain or irritation at the site of an injury truly is inflammatory in nature, both the macroscopic and microscopic signs should be evident – but microscopic signs aren’t easily detectable.
Sensations like pain, redness, and swelling are easy to observe, but you need to actually look at tissue under a microscope or with high-tech biology equipment to see the cellular markers of inflammation.
As you might guess, runners and other athletes with mild or moderate overuse injuries aren’t too keen on letting researchers put a slice of their Achilles tendon or plantar fascia under a microscope in the name of science.
Partly because of the difficulty of observing the cellular signs of inflammation, the inflammatory theory of running injuries has been popular for quite a while. Problems with it have arisen only recently, as doctors and researchers have begun to thoroughly investigate the root causes of overuse injuries.
Treatments and rehabilitation vs inflammatory model
Using tissue samples taken from patients with chronic tendon or plantar fascia injuries who undergo surgery (and are hence being sliced open anyhow), recent studies have demonstrated a lack of inflammatory markers at the cellular level. Instead, what they observe in injured tissue under a microscope is profound damage and degeneration in the microscopic structure of the tissue.
Other research has highlighted the relatively poor track record of anti-inflammatory treatments like non-steroidal anti-inflammatory drugs and corticosteroid injections. And the most promising emerging treatments for soft-tissue overuse injuries don’t appear to address inflammation at all.
The eccentric heel drop exercise developed for Achilles tendonitis and the decline squat exercise developed for patellar tendonitis both focus instead on attempting to fix the structure of the tendon through controlled eccentric stress, and the most successful rehab programs for knee injuries like IT band syndrome and patellofemoral pain syndrome (runner’s knee) are focused on improving hip strength and coordination to reduce damaging stresses on the knee from poor running mechanics. In essence, as our very own Matt Phillips pointed out, we need to think prehab rather than rehab!
More intensive emerging treatments like shockwave therapy or nitroglycerin patches don’t focus on reducing inflammation either—in fact, often the goal is to induce controlled inflammation or increase bloodflow, targets anathema to an inflammatory model of injury. This is in keeping with the fact that some researchers believe that inflammation is a helpful and necessary component of recovery.
Final notes and specific recommendations for rehabbing your injuries
So, knowing that the inflammatory model of injury is unsatisfactory, how does this inform the way we think about treating and rehabbing injuries?
First, it should give us pause when evaluating any new treatment, therapy, or device which claims to reduce inflammation.
Second, we should also acknowledge that many (if not all!) injuries are painful because there is real, physical damage to something in your body.
Instead of icing a bit or taking some ibuprofen before you run, your recovery plan should be more cautious and allow your body time to repair the damaged tissue.
While this might include taking time off from running, it might also be simply modifying your running schedule to put less stress on an injured area.
Finally, it means that you should concentrate your rehabilitation efforts on the treatments that are most likely to help with your particular injury (typically specific strength exercises and sometimes stretches) and put less emphasis on traditional anti-inflammation tactics like icing, anti-inflammatory drugs, compression wraps, and elevation.
Though we need scientific research on individual treatments to explicitly rule out specific treatments for specific injuries—for instance, the absence of inflammation in connective tissue injuries doesn’t necessarily mean we should throw out the notion that icing, for example, can be useful—an overall model of understanding the biology that underpins an overuse injury can help you prioritize your recovery plan.
Login to leave a comment
Latest Running News

The Soccer Player Who Became Austria’s Olympic Marathon Record Holder
Most Olympic marathoners spend their youth focused on running. They join track clubs, compete in national championships, and pursue the sport from an early age.
Julia Mayer’s journey was very different.
Today, Mayer is Austria’s marathon record holder, a multiple national record holder on the roads, and an Olympian. Yet for much of her athletic life, running was not her primary sport.
For 16 years, she played soccer.

Then she discovered something that would change her life.
“I noticed that I was really fast in the fun runs and that it was really, really fun,” Mayer said when reflecting on her transition from soccer to distance running.

What began as curiosity quickly became a passion. She eventually made the bold decision to leave soccer behind and focus entirely on running. It was a move that surprised many people around her, but Mayer believed she had found her true athletic calling.
The decision proved to be the right one.
Within a few years, Mayer developed into one of Europe’s top marathon runners. Her steady improvement carried her from local races to the international stage, where she began rewriting Austria’s record books.
She now holds Austrian records in the marathon, half marathon, and road 10K. Her marathon best of 2:26:08 established her as the fastest female marathoner in Austrian history. Her performances in the half marathon and 10K have further cemented her place among the country’s all-time great distance runners.
Her rise culminated with qualification for the 2024 Olympic Games in Paris.
Competing in the Olympic marathon represented the realization of a dream. On one of the most challenging marathon courses ever used for the Olympics, Mayer ran courageously against the strongest field in the world and finished 55th in her Olympic debut.
Behind the scenes, success has come through extraordinary dedication. During marathon preparation, Mayer trains twice a day and covers approximately 200 kilometers, or 124 miles, each week. The workload demands discipline, patience, and a deep commitment to continuous improvement.
What makes her story especially inspiring is not simply the records or the Olympic appearance.
It is the fact that she found her greatest talent later than many elite runners.
In a sport where athletes are often identified at a young age, Mayer’s journey serves as a reminder that potential does not always reveal itself early. Sometimes it takes years of experience, a willingness to try something new, and the courage to follow a different path.
The former soccer player who once chased a ball across a field is now chasing history on the roads of Europe.
And according to those closest to her, her best performances may still be ahead.
For runners of every age and ability, Julia Mayer’s story delivers a powerful lesson: it is never too late to discover what you are capable of.
From soccer player to Olympian, her journey proves that remarkable achievements can begin when least expected.
by Boris Baron
Login to leave a comment

Megan Keith Rewrites Scottish History with Stunning 3000m Record in Oslo
Megan Keith produced the performance of her career in Oslo on Thursday night, shattering one of Scotland’s longest-standing distance running records and cementing her place among Britain’s greatest female 3000m runners.

The 24-year-old clocked a sensational 8:28.35 over 3000m, breaking the Scottish outdoor record that had stood for nearly four decades. In doing so, Keith eclipsed the previous mark of 8:29.02, set by Scottish legend Yvonne Murray back in 1988, ending a record reign that had lasted 38 years.

Keith’s breakthrough run was more than just a national record. The performance also propelled her to third on the UK outdoor all-time list, placing her behind only two of Britain’s most celebrated distance runners — Paula Radcliffe, who leads the rankings with 8:22.20, and Laura Weightman, whose 8:26.07 remains the second-fastest outdoor mark by a British woman.
The significance of Keith’s achievement is amplified by the calibre of athletes she now joins in the record books. For decades, Murray’s mark stood as one of Scottish athletics’ most untouchable records, surviving generations of elite competitors. Keith has now succeeded where many outstanding runners have fallen short, announcing herself as one of the leading distance talents in British athletics.
Her time also compares favourably with the best performances produced indoors. Olympic medallist Laura Muir ran 8:26.41 indoors in Karlsruhe in 2017, underlining just how exceptional Keith’s outdoor effort in Oslo truly was.
The run continues a remarkable rise for the Scottish star, whose progression over recent seasons has transformed her from a promising prospect into a genuine force on the international stage. Running with confidence and composure against elite competition, Keith demonstrated both the speed and endurance required to challenge the very best in Europe and beyond.
With the World Championship season gathering momentum, Keith’s record-breaking display sends a powerful message. Not only has she etched her name into Scottish athletics history, but she has also established herself as a serious contender in one of the sport’s most competitive events.
In Oslo, Megan Keith did far more than break a record. She ended a 38-year wait, climbed into the upper echelon of British distance running, and delivered a performance that may prove to be a defining moment in her career.
by Erick Cheruiyot for My Best Runs.
Login to leave a comment

Gill Continues Encouraging Comeback with Marseille 800m Victory
British middle-distance talent Phoebe Gill took another significant step forward in her return to top form, producing a determined victory over 800 metres at the Meeting de Marseille in France on Wednesday.

Competing in challenging, wind-affected conditions, the 19-year-old demonstrated both resilience and composure as she held off a late charge from Switzerland's Veronica Vancardo to secure the win in 2:00.81. Vancardo finished just three hundredths of a second behind in 2:00.84, underlining the fiercely contested nature of the race.
While the margin of victory was narrow, the result represented another encouraging milestone for Gill as she continues to rebuild momentum following her injury setback. The young Briton showed impressive race awareness and strength in the closing stages, maintaining her advantage despite the difficult conditions that made fast running a challenge throughout the evening.

The Marseille triumph adds to a growing body of evidence that Gill is steadily progressing toward her best form. Earlier in her comeback campaign, she clocked 2:01.50 for 800m in Bydgoszcz before demonstrating her versatility with a strong 4:05.53 performance over 1500 metres at the BMC Grand Prix meeting in Trafford.
Those performances have highlighted not only her improving fitness but also her ability to compete across multiple distances as she carefully builds her season. The Marseille victory now provides further confirmation that the European junior star is moving in the right direction.
Gill emerged as one of Britain's most exciting middle-distance prospects through a series of breakthrough performances as a teenager, earning widespread recognition for her fearless racing style and remarkable maturity. Injury temporarily interrupted that upward trajectory, but her recent results suggest she is steadily rediscovering the form that made her one of the sport's brightest young talents.
With each race, the signs of progress become increasingly evident. Winning in difficult conditions and under pressure from a quality field is often a stronger indicator than a fast time alone, and Gill's latest success demonstrated exactly those qualities.
As the summer season gathers pace, the Marseille victory offers another confidence boost for the British teenager, whose return continues to gain momentum. If her recent progression is any indication, Gill could soon find herself back among the leading names on the European middle-distance circuit.
by Erick Cheruiyot for My Best Runs.
Login to leave a comment

Ja’Kobe Tharp Shatters World Record with Historic NCAA Hurdles Performance
The NCAA Track and Field Championships delivered a moment few could have predicted as Ja’Kobe Tharp produced one of the most astonishing performances in the history of sprint hurdling, rewriting the record books in spectacular fashion.

Competing in the opening round of the men’s 110-meter hurdles, the Auburn star stunned the athletics world by clocking an incredible 12.75 seconds, becoming the first athlete ever to break the 12.80-second barrier. In doing so, he eclipsed the long-standing world record of 12.80 set by Aries Merritt in 2012, a mark that had stood as one of the sport’s most revered achievements for more than a decade.

What makes Tharp’s breakthrough even more remarkable is the scale of his improvement. Entering the championships, the defending NCAA and U.S. champion had recorded a season-best of 13.05 seconds. Yet under the brightest spotlight, he unleashed a performance that exceeded every expectation, slicing an extraordinary 0.26 seconds from his personal best in a race that instantly became one of the greatest ever run.
The achievement sent shockwaves throughout the track and field community. While Tharp arrived in Eugene as one of the leading contenders for the NCAA title, few envisioned a performance capable of redefining the limits of the event. Instead, the American hurdler delivered a race for the ages, combining flawless technique, explosive speed, and impeccable rhythm from the first hurdle to the finish line.
The historic run not only secured his place in athletics history but also transformed the outlook of the championship. With the world record now in his possession, Tharp advances to the final as the overwhelming favorite, carrying momentum that could make an already unforgettable weekend even more extraordinary.
For years, the 12.80 barrier appeared untouchable. On a stunning day at the NCAA Championships, Ja’Kobe Tharp proved otherwise, producing the kind of performance that reminds fans why sport remains so unpredictable. In a matter of seconds, he turned a routine qualifying round into a landmark moment that will be remembered for generations.
The world record no one saw coming is now a reality—and Ja’Kobe Tharp is the man who changed history.
by Erick Cheruiyot for My Best Runs.
Login to leave a comment

Lutkenhaus Delivers Stunning Upset as Teenage Star Edges Olympic Champion in Oslo
A new chapter in middle-distance running may have begun in Oslo after American teenager Cooper Lutkenhaus produced one of the most remarkable performances of the season, narrowly defeating reigning Olympic champion Emmanuel Wanyonyi in a thrilling men's 800m contest at the Diamond League meeting.

The 17-year-old sensation shocked a world-class field by crossing the finish line first in a race that came down to the smallest of margins. After an intense battle over the final metres, Lutkenhaus held off Wanyonyi by just one hundredth of a second, producing a dramatic finish that left the packed stadium in disbelief.

From the opening lap, the pace was relentless as the leading contenders positioned themselves for a fierce showdown. As the athletes entered the home straight, Wanyonyi appeared poised to unleash his trademark finishing kick. However, Lutkenhaus refused to be intimidated, matching the Olympic champion stride for stride before producing a perfectly timed lean at the line to secure a historic victory.
The result marks a breakthrough moment for the young American, who continues to establish himself as one of the brightest talents in global athletics. Defeating an Olympic champion at a Diamond League event is a feat many athletes spend entire careers pursuing, yet Lutkenhaus achieved it before reaching adulthood.
For Wanyonyi, the narrow defeat does little to diminish his status as one of the world's premier 800m runners. The Kenyan once again demonstrated his exceptional class and competitiveness, pushing the race to a world-class standard and forcing his young rival to deliver the performance of a lifetime.
Beyond the result itself, the race offered a glimpse into what could become one of the sport's most exciting rivalries in the years ahead. With established stars and emerging talents now pushing each other to new heights, the men's 800m continues to evolve into one of athletics' most captivating events.
On a memorable night in Oslo, the spotlight belonged to Cooper Lutkenhaus. At just 17 years old, he stood toe-to-toe with an Olympic champion and emerged victorious, announcing himself to the athletics world in spectacular fashion.
by Erick Cheruiyot for My Best Runs.
Login to leave a comment